Screening for Hydroxychloroquine Retinopathy in 2026: How Combined-Density Visual Field Testing Addresses the AAO’s Revised Recommendations
The updated AAO guidelines call for visual field strategies that cover both parafoveal and pericentral regions in a single test. RadiusXR’s High-Density Central (HDC) exam was designed to do exactly that.
RadiusXR
•
A Decade-Overdue Update
In November 2025, the American Academy of Ophthalmology published its Recommendations on Screening for Hydroxychloroquine Retinopathy (2025 Revision) in Ophthalmology, the first major update to these guidelines since 2016. Authored by Marmor, Ahn, Ehlers, Melles, Mieler, Sarraf, and Yussuf on behalf of the AAO, the revised statement reflects a decade of new evidence on the prevalence, patterns, and progression of hydroxy-chloroquine (HCQ) retinal toxicity.
The core screening recommendations remain anchored to spectral-domain OCT and wide-pattern fundus autofluorescence (FAF) as the primary tools. However, the revised guidelines significantly expand the role of automated visual fields as a secondary and confirmatory technique and, in doing so, highlight a long-standing practical gap in how clinicians approach visual field–based hydroxy-chloroquine screening.
The Screening Challenge: Two Patterns, One Patient
HCQ retinopathy does not present uniformly. Patients of European descent most often develop parafoveal damage; photoreceptor loss is concentrated in a ring close to fixation. Patients of East Asian descent more commonly show pericentral damage extending further from the fovea, near or beyond the arcades. Black patients and those from the Indian subcontinent may present with a mixed pattern. The revised AAO recommendations are explicit: screening examinations should look for both patterns.
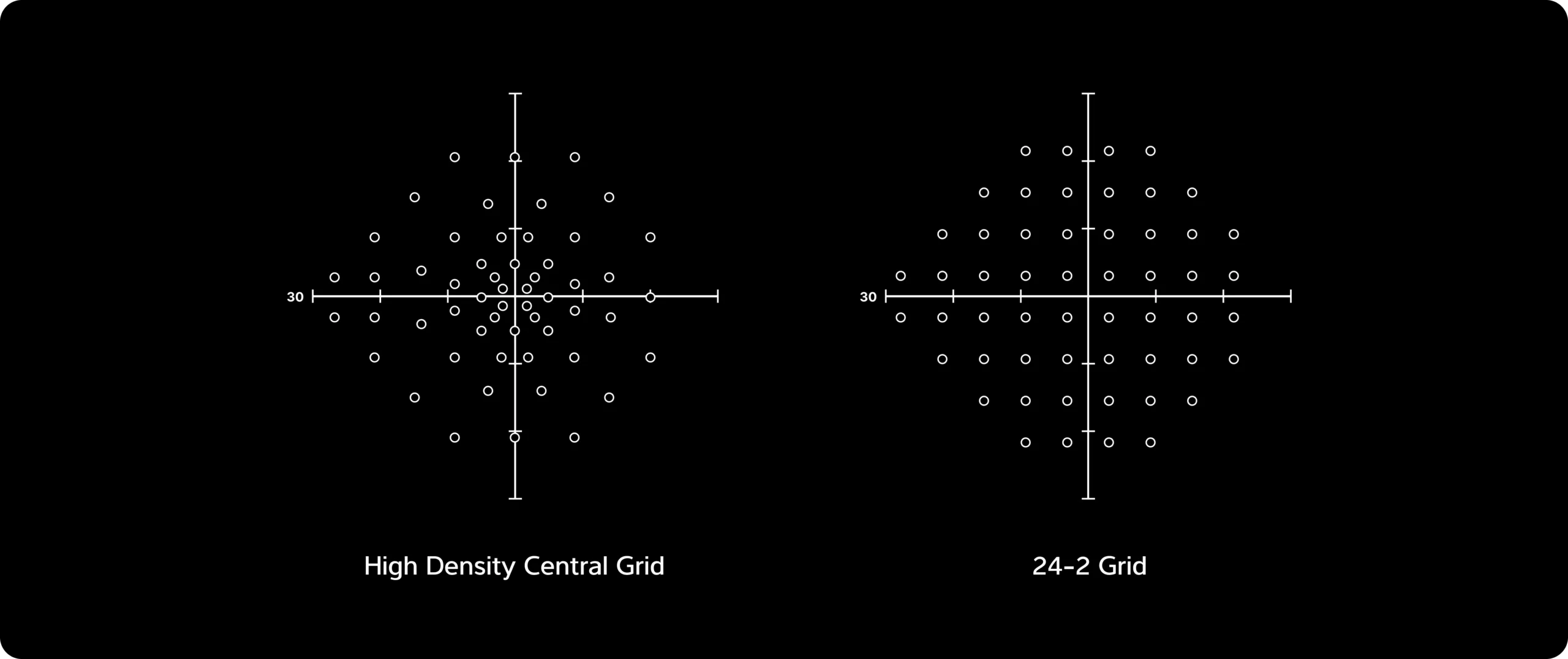
This has practical implications for visual field testing. The traditional 10-2 pattern offers dense 2° spacing ideal for detecting parafoveal scotomas, but its coverage stops short of pericentral regions. The standard 24-2 pattern reaches the periphery but lacks the central density to catch subtle parafoveal defects. Historically, clinicians who wanted both had to run two separate tests, doubling chair time, patient burden, and technician workload.
The revised AAO guidelines acknowledge this gap directly, noting that “newer VF algorithms such as 24-2C can screen both parafoveal and pericentral regions simultaneously” and that effective screening “can be accomplished now with a single test using one of several algorithms … that add central points to a wider test pattern.”
Introducing the High-Density Central (HDC) Test
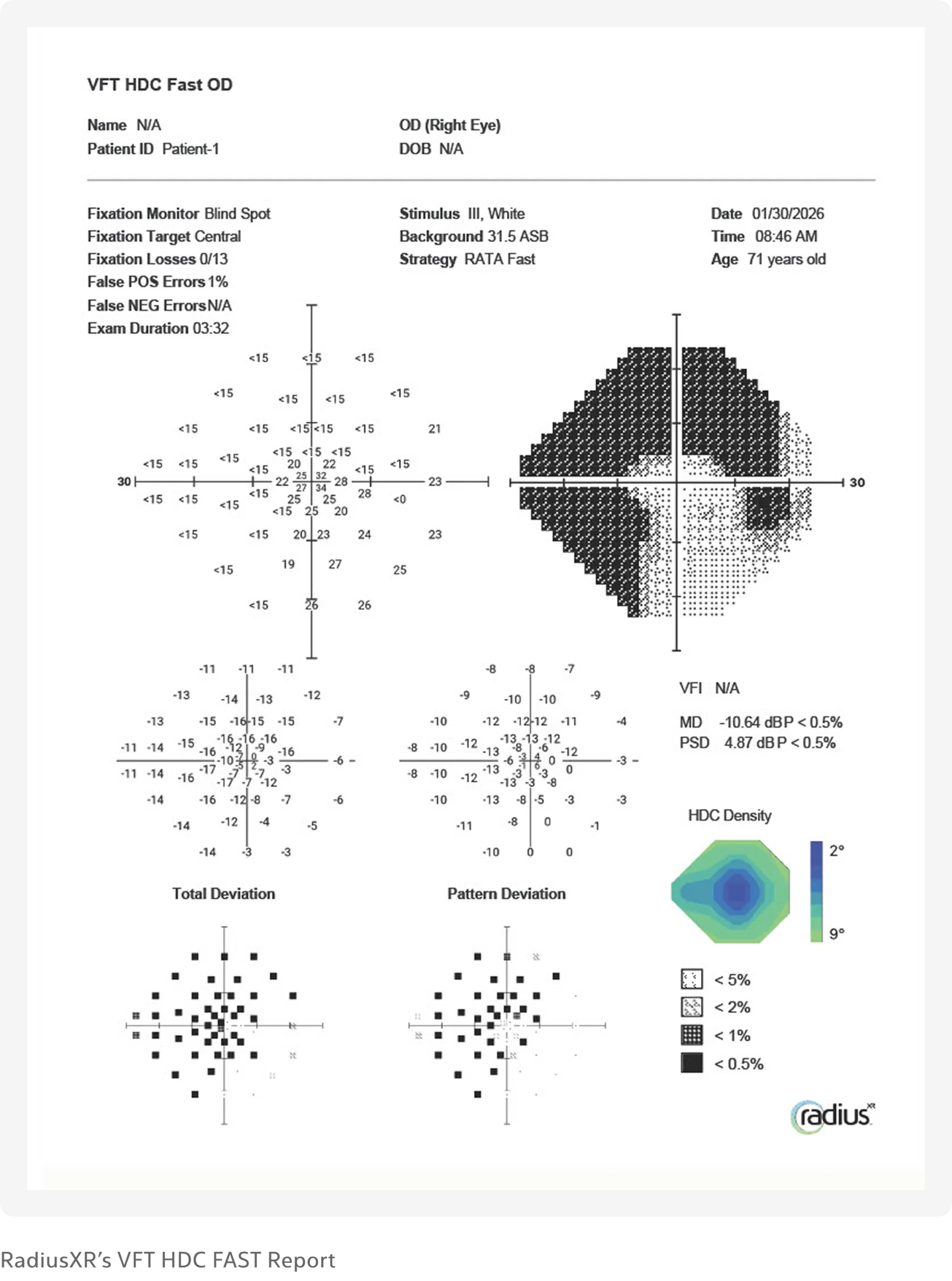
The High-Density Central (HDC) test from RadiusXR was designed to address precisely this clinical need. The HDC merges the efficiency of the 24-2 RATA Fast algorithm with the dense central sampling of the 10-2 RATA Fast, delivering both in a single, combined exam.
How It Works
The HDC employs 55 test points across an adaptive density grid. At the center, spacing is at 2°, matching the resolution of a 10-2 pattern where parafoveal defects first emerge. Moving outward, spacing gradually increases to 9°, preserving the peripheral reach needed to detect pericentral and extramacular pathology. The result falls between a 10-2 (68 points) and a 24-2 (54 points) in total point count, but critically covers both clinical zones of interest in a single acquisition.
Despite this expanded coverage, the HDC maintains the same rapid test duration as a standard 24-2 RATA Fast exam. There is no additional time cost to the patient or clinic.
“The HDC merges the efficiency of the 24-2 RATA Fast algorithm with the dense central sampling of the 10-2 RATA Fast, delivering both in a single, combined exam.”
Clinical Relevance to HCQ Screening
The HDC’s design maps directly onto the AAO’s updated screening framework:
Parafoveal sensitivity: The 2° central spacing provides the resolution needed to identify early parafoveal scotomas characteristic of European-pattern toxicity, the subtle defects that a standard 24-2 may miss.
Pericentral coverage: The expanded peripheral grid captures the broader distribution seen in East Asian- and mixed-pattern disease, regions that a 10-2 alone cannot reach.
Workflow efficiency: By combining both strategies into a single exam, the HDC eliminates the need to order, schedule, and administer separate 10-2 and 24-2 tests. This is particularly meaningful for patients already burdened by the cumulative demands of chronic disease management.
Why This Matters Now
HCQ remains the preferred treatment for systemic lupus erythematosus and is widely used for rheumatoid arthritis, sarcoidosis, and related autoimmune and dermatologic conditions. Its use is expanding into diabetes mellitus, heart disease, and adjunct cancer therapy. The patient population requiring HCQ screening is growing, not shrinking.
At the same time, the AAO’s revised guidelines raise the bar on what constitutes adequate screening. The recommendations call for annual screening with OCT and FAF for patients on hydroxy-chloroquine, with visual fields serving as a confirmatory tool when subtle or inconclusive signs are noted on objective testing. The guidelines specifically note that VF changes should prompt retesting within a few months to ensure consistency and should be compared with OCT and FAF findings.
In this context, having a visual field strategy that can screen both patterns of damage in a single sitting without sacrificing test speed is not a convenience. It is a clinical efficiency that helps practices meet the AAO’s more comprehensive screening standard without adding operational burden.
Beyond HCQ: Additional Clinical Applications
While the HDC’s combined-density design is particularly well-suited to HCQ screening, its clinical utility extends to several other conditions where central and pericentral visual field detail is critical:
Normal tension glaucoma, where early damage often appears close to fixation and may be missed by standard 24-2 testing.
Defects near fixation, including central and paracentral scotomas, threaten visual acuity.
Combined central and peripheral loss, where a single comprehensive map is more clinically useful than two separate exams.
Neuro-ophthalmic conditions with macular or foveal sparing, where detecting the boundary between preserved and damaged regions requires dense central sampling within a broader field context.
Implications for Practice
The AAO’s revised guidelines underscore a practical reality: compliance with HCQ screening recommendations has historically been far from universal. The guidelines note that “a significant subset of patients take more than the recommended dose of HCQ or fail to undergo baseline and proper screening examinations.” Simplifying the visual field component of screening by reducing it to a single, combined-density exam that requires no additional chair time removes one barrier to guideline adherence.
“A significant subset of patients take more than the recommended dose of HCQ or fail to undergo baseline and proper screening examinations.”
For practices that have traditionally deferred VF testing in hydroxy-chloroquine screening or have limited the exam to a standard 24-2, the HDC offers a path to more comprehensive coverage without disrupting workflows. For practices already running both 10-2 and 24-2 tests on these patients, the HDC consolidates that effort into a single exam.
Conclusion
The 2025 revision of the AAO’s HCQ screening recommendations reflects a more nuanced understanding of retinal toxicity patterns and a more demanding standard for clinical screening. Visual field testing, while secondary to OCT and FAF, remains an important confirmatory tool, and the guidelines now explicitly call for strategies to assess both the parafoveal and pericentral regions.
The HDC test from RadiusXR was purpose-built for this clinical moment: a single, fast, combined-density visual field exam that delivers 10-2–level central resolution and 24-2–level peripheral reach. For clinicians seeking to align their screening protocols with the AAO’s updated guidance, the HDC offers a practical, efficient path forward.
References
Marmor MF, Ahn SJ, Ehlers JP, Melles RB, Mieler WF, Sarraf D, Yussuf IH, for the American Academy of Ophthalmology. Special AAO Report: Recommendations on Screening for Hydroxychloroquine Retinopathy (2025 Revision). Ophthalmology. 2026;133:439–450.
RadiusXR is transforming visual field testing and eye care with an advanced digital platform that enables unrivaled patient access, streamlines operations, and creates more confidence at the point of care. Our clinically validated portable platform integrates seamlessly into existing systems, with customized software and cloud technology to securely manage data and a lightweight, purpose-built headset. With our advanced wearable technologies, we continue developing disruptive technologies that challenge the healthcare status quo.